
If you’ve ever blamed a sleepless night, a sudden fever, or a week of unexplained misery on your baby’s teeth, you’re not alone. But you might be surprised how little of that is actually down to new teeth coming through.
Teething is one of the most mythologised milestones of early parenthood, surrounded by folklore, well-meaning but scientifically shaky advice, and a surprisingly rich body of research that most of us never hear about.
In the latest episode of the Science Baby Podcast, we dig into the fascinating biology of teething, from how teeth actually emerge (hint: not how you think) to what genuinely helps a distressed baby.

What’s Actually Happening in Your Baby’s Mouth
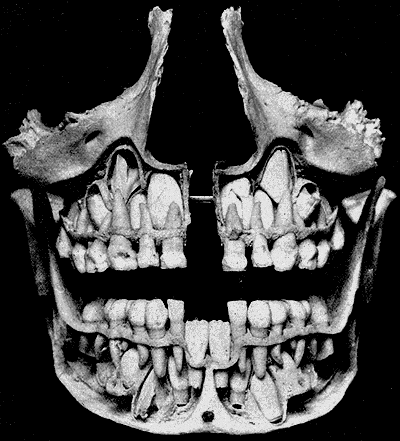
Here’s something that surprises most parents: your baby isn’t born without teeth: they’re born with a full set of 20 milk teeth already formed inside their jaw, waiting. Tooth development begins remarkably early in pregnancy, with the first tooth buds forming at around six weeks’ gestation. By birth, all of those primary teeth exist as mineralised structures sitting beneath the gum line, some of them already quite close to the surface.
Do teeth really ‘cut’ through the gums?
The old-fashioned term ‘cutting teeth’ is vivid, but it’s not quite accurate. When a tooth is ready to emerge, the body releases hormones that trigger programmed cell death in the gum tissue above it. The cells essentially dissolve in a controlled way, creating a natural opening, a bit like a little buttonhole, for the tooth to pass through without causing real damage. This is why teething is rarely accompanied by significant bleeding. Evolution has solved the problem of repeated tissue breach in a young, vulnerable organism in the most sensible way possible.

How do teeth actually move upward? (Science still isn’t entirely sure)
You might assume that the mechanism by which teeth rise through the jaw is well understood by now. It isn’t. It’s not exactly ethical to pull apart an infant’s jaw just to see how things are working.
Some thought that the tooth’s root grows downward and pushes it up. Others said growing bone around the tooth acted as a piston. The most entertainingly wrong was the ‘cushioned hammock theory’ which proposed a trampoline-like structure of soft tissue beneath the tooth bouncing it upward.
The current best understanding is that the periodontal ligament – fibres attached to the sides of the tooth’s root – peffectively hauls the tooth upward. Ironically, this makes the cushioned hammock theory not entirely wrong in spirit, just wrong in the specifics. Tooth eruption, it turns out, is driven more by soft tissue than by hard bone.
Timing and Order: What to Expect (and When Not to Panic)
Like so much with baby development, your child will get their teeth at their own pace. Most babies get their first tooth at around six months, but the normal window is wide. Anywhere from before four months to after twelve months is considered typical by the NHS.
The order of apperance usually goes:
- lower central incisors (the two front bottom teeth),
- upper central incisors (the two front top teeth)
- lateral incisors top and bottom
- first molars top and bottom
- canines top and bottom
- second molars top and bottom
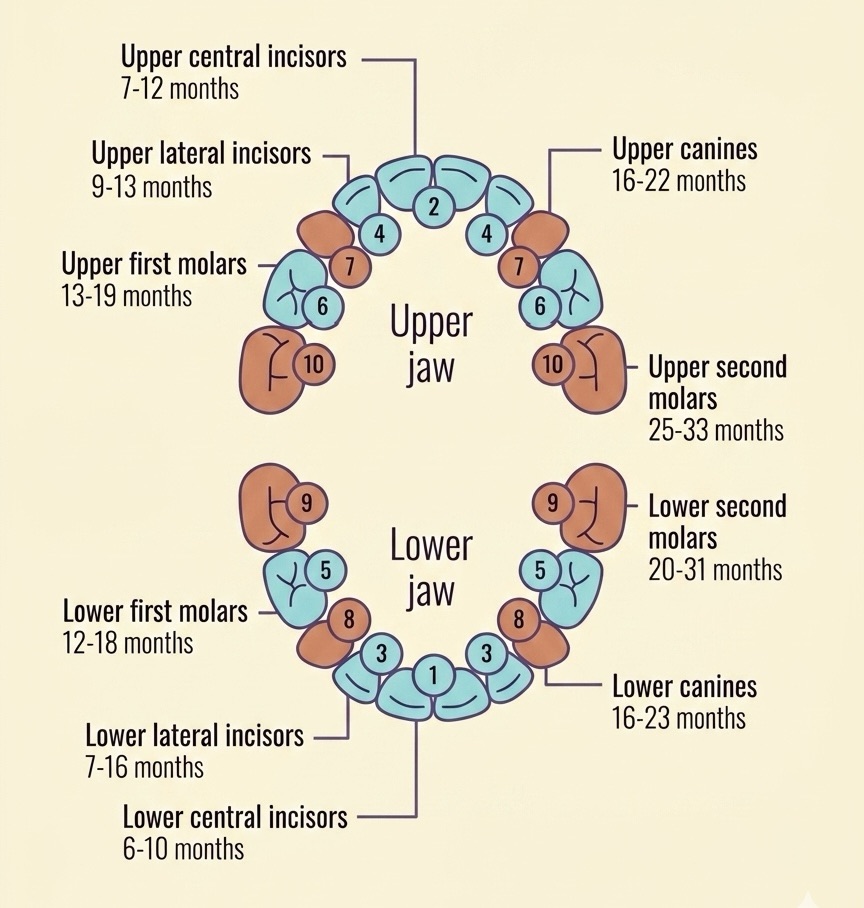
The order has a logic to it that mirrors a baby’s growing dietary needs. Since they’re only having (and only need) milk for the first few 4 to 6 months of their lives, they’re born gummy. Then, teeth start to come through conveniently when most parents wean.
The biters come first, equipping a baby for the initial stages of eating solid food. Then come the grinders as a diverse range of foods needs chewing, followed eventually by the canines that are used for the relatively advanced act of tearing food.
Baby nutrition and dental development are deeply intertwined.
Why does timing vary so much between babies?
Between 70 and 95% of the variation in when and in what order teeth erupt is genetic. If you were a late teether, there’s a good chance your baby will be too. Environmental factors account for a smaller but meaningful proportion.
Intriguingly, some research has found that babies tend to teeth earlier when mothers had higher ster levels during pregnancy (cortisol being the body’s primary stress hormone). Smoking during pregnancy and lower socioeconomic circumstances have also been associated with earlier tooth eruption.
One hypothesis is that this hormone signals that the environment the baby is born into is going to be one of stretched resources, so the baby’s biology adapts to be less dependent earlier on. On the other hand, nutritional deficiencies can delay or impair tooth mineralisation.
Why Do Milk Teeth Fall Out? The Case for Deciduous Teeth
Once you’ve watched your baby suffer through weeks of teething misery, it can feel particularly cruel to learn that all those teeth are going to fall out anyway. But there’s a very good reason for it.
Teeth, unlike bones, are fixed structures. Once formed, they don’t grow. (And they can’t be affected by things like mineral deficiencies in pregnancy and breastfeeding which eats away at the calcium in a mother’s bones).
Adult teeth are simply too large to fit in a baby’s jaw, and a jaw that still has years of growing ahead of it can’t accommodate permanent teeth without significant misalignment. So the body’s solution is a two-set system: a miniature first set (the deciduous teeth) sized for a small jaw, which hold the space open and guide the permanent teeth into correct position when the jaw is finally ready for them.
This also has an important implication for dental care. Even though milk teeth will eventually fall out, they are not expendable. They preserve the spacing that adult teeth depend on, support the development of normal speech (the tongue relies heavily on the teeth when forming many sounds), and contribute to healthy jaw development.
Losing a milk tooth prematurely to decay can cause crowding of permanent teeth years later. The NHS provides free dental care for children, and the first check-up is recommended around the time the first tooth appears.
Teething Symptoms: What’s Real and What’s a Myth
Teething does cause real symptoms, but parents often attribute far more to it than is actually justified.
For instance, teething itself doesn’t actually cause a fever!
Here’s what the evidence says:
- Sore, red gums: where the tooth is pushing through is genuine inflammation.
- Excessive drooling: The gum inflammation triggers increased saliva production, and babies lack the swallowing coordination to keep up with it.
- Loose stools and nappy rash: All that extra saliva gets swallowed too, and can make stools more acidic. This is often mistaken for a gastrointestinal illness.
- Increased chewing and mouthing: Babies instinctively apply counter-pressure to the gums. This is why they’ll gnaw on anything within reach.
- Mild temperature rise: Teething may raise body temperature very slightly but not to fever level. A temperature of 38°C or above is not a teething symptom and should be assessed by a doctor.
- Fever: NOT caused by teething itself. During the teething age bracket (roughly six months to two years), babies are highly susceptible to infections. And since teething babies are constantly putting objects in their mouths, coincident infection is extremely common. The fever is real; the teething is just a bystander.

What Actually Helps (and What Doesn’t)
Evidence-based relief
The sensation of teething appears to be closer to itching or pressure than to sharp pain which explains why pressure from chewing and cooling provide relief. Effective approaches include:
- Chilled (not frozen) teething rings: cold reduces inflammation; freezing risks damaging gum tissue.
- Clean finger massage of the gums: direct pressure on the inflamed area.
- Chilled solid foods for babies over six months, such as a cold wedge of cucumber or a crust of bread (always supervised).
- Infant paracetamol or ibuprofen (for babies over the appropriate age threshold) when discomfort is clearly significant.
What the evidence doesn’t support
Amazingly, teething gels have very little scientific evidence behind them. The studies that exist are generally small and methodologically weak. Any relief babies appear to experience is likely attributable to the gum massage involved in application, and the cooling sensation of the gel itself, rather than any active ingredient.
They are not harmful in themselves, but parents should not expect them to be reliably effective.
Amber teething necklaces should be avoided entirely. There is no evidence they provide any benefit, and they pose a genuine strangulation and choking hazard. The same applies to any necklace or cord worn around an infant’s neck. The NCT and NHS both advise against them.

Caring for Your Baby’s Teeth: Why It Matters More Than You Think
It can feel tempting to be relaxed about milk tooth hygiene on the grounds that they’re going to fall out anyway. This is understandable, but sadly wrong.
The NHS recommends brushing as soon as the first tooth appears, twice a day, using a tiny smear of fluoride toothpaste (about the size of a grain of rice for babies, a pea-sized amount from age three).
Particular vigilance is needed once the molars arrive. Their bucket-shaped surfaces and position at the back of the mouth make them highly vulnerable to decay, especially overnight, when saliva production drops and pooled milk or food sits undisturbed on the tooth surface. Once those back teeth are in, cleaning them before sleep becomes critically important.
Listen to The Episode
👉 You can watch and listen to the latest episode right here:
Or find The Science Baby Podcast on your favourite podcast app.
Join the Science Baby Community
We’d love to hear what you think about this episode, and the podcast in general!
Leave us a review, share this episode with a fellow parent, or drop us a message with the topics you’d love us to cover.
And make sure to follow us on Instagram, Facebook, TikTok or YouTube to make sure you never miss an update.
Read More
For further reading on everything covered in this episode, the following sources are reliable and accessible:
- NHS: Baby Teething Symptoms
- NCT: Teething in Babies and Young Children
- NHS: Looking After Your Baby’s Teeth
- British Dental Journal: How Do Teeth Erupt?
- OUP Blog: Where Do Our Teeth Come From?
- Wikipedia: Tooth Eruption (overview of eruption theories)
- Children’s Hospital Los Angeles: A Parent’s Guide to Teething
- Better Health Channel: Teeth Development in Children
- NCH/Pediatrics study: Teething Unlikely to Cause Serious Symptoms (Reuters/Ramos-Jorge)
- Gorgie Road Dental: Why Baby Teeth Matter More Than You Think








Leave a comment